
Cognitive Behavioral Therapy is the combination of two theories and therapies to overcome a wide range of mental health conditions, most notably anxiety and depression. CBT has been studied and researched for years and is considered an Evidenced Based Practice which is a testament to its effectiveness when done correctly.
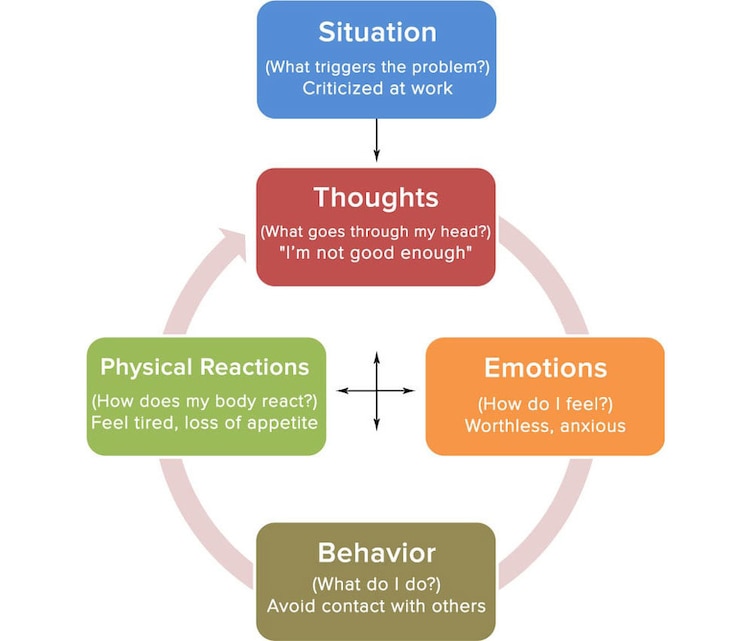
The “cognitive” part of CBT is based on the assumption that thoughts create attitudes and then attitudes drive behavior. So the intervention is to teach someone to think about their thoughts (in order to change them). One is unable to change what he/she is unaware of. So the first step is having someone identify their thoughts by keeping a journal and expressing their thoughts in the session. When someone is able to think about their thoughts (meta-cognition), then they can examine the thoughts. When someone is able to examine their thoughts, then he/she is able to weigh the thought to determine if it is true or not and decide whether they want to substitute a more positive, constructive thought. Children often pick up distorted views of themselves and how they fit in the world. By examining their thoughts now, adults can choose which thoughts are true and which thoughts are no longer beneficial to them.
However, CBT is not popular “positive thinking” which can deny problems and challenges in life. CBT attempts to help a person see things in a more balanced view, and yes, tip the scales towards positive thinking without discounting that there is a challenge. It relies more on positive problem solving than denial of problems.
Another underlying assumption for CBT is that it is not the event that creates anxiety, it is the way a person perceives the event. CBT examines Automatic Thoughts and underlying schemas.
One illustration of this point I like to discuss in session is to ask the person to imagine three drivers, driving the same type of car behind another car. They have the same weather conditions and road conditions and each one briefly takes their eyes off the road to find their ringing cell phone underneath clothes on the seat next to them. And as you guessed, the car in front stops and they crash into the car in front.
Driver 1 gets out of his car and thinks “I’m an idiot”. He feels incompetent and unworthy and degrades himself for this accident. He doesn’t believe he should drive anymore. So he doesn’t learn how to be a better driver.
Driver 2 gets out and yells at the driver in front “You idiot! If you hadn’t stopped I wouldn’t have run into you!” He doesn’t get ulcers because he believes everyone else has the problem. But he doesn’t learn from it either. He continues to make mistakes.
Driver 3 has the exact same accident, gets out of his car, feels bad about what happened and takes responsibility but it doesn’t crush him. He decides to learn from it. He vows to never take his eyes off the road while driving. He might even enroll in a driving class, etc. He learns from his accidents or mistakes. It’s the exact same scenario but each one walks away thinking and doing something different. Why?
In session, this example leads to discussion on ATs and underlying schemas that everyone has. For some these can be constructive and for others destructive. Therapy includes uncovering and examining one’s underlying schema, their view of the world and of themselves. The goal is to change the ATs by changing the schema so that it generates balanced, resilient thinking patterns (if the person wants to change).
The “Behavior” part of CBT relies on researchers like Pavlov and B.F. Skinner. Behavior Therapy is also an EBP. Like CBT, there are many techniques considered as Behavior Therapy. Exposure therapy, a technique in BT, when done by a trained professional, is still considered the treatment of choice for phobias and other anxiety disorders.
Behavior Therapy takes a different approach than CBT. It’s underlying belief is that when one changes one’s behavior then the thinking will change. BT is not interested much in how one is thinking when they come into therapy. They analyze the behavior that is problematic and focus on what the client wants to change.
The goal is to change a behavior and then the thinking will change over time. A standard goal when working with people who are depressed is to have them do activities. Depression robs people of their energy and motivation. BT believes that a person may have to force themselves to move in the beginning and then that movement is reinforced by positive feelings and then any behavior that is reinforced is more likely to be repeated. Over time it becomes a habit and the person then begins to justify why they did it. And this leads to more of the positive behavior.
Two main branches of BT are operant learning and classical conditioning. This will be discussed more in a future article.
The point is that both of these therapies, cognitive and behavioral therapies are powerful in the change process individually. When used together they can produce change in a relatively short time frame. But the elements for change that are needed include motivation, effort and doing homework. Both of these approaches and CBT do believe in self-determination and respect for the client. A therapy may be wonderful, but if the client doesn’t buy into it and is not willing to do work outside of the sessions, then little change will be effected.
The CCP is a short-term counseling program through MCCS- Marine and Family Programs, bldg. 218, which helps people overcome and/or manage problems as a result of anxiety or depression or grief and loss, adjustment issues, parenting issues, couples/relationship problems, etc. It is available to Active Duty Military and their dependents. Eligible people who live off base can still use the counseling services for free on base. The CCP is also open for retirees and their dependents. If you have questions or want more information, please call Jim Maher at 760-577-6533.
References:
Cognitive Therapy:
• http://psychology.about.com/od/psychotherapy/a/cbt.htm
• psychologydegreeguide.org/cognitive-behavioral-therapy
• Guide_to_Brief_CBTManual.pdf (www.mirecc.va.gov/visn16/docs/therapists)
Behavioral Therapy:
• http://psychology.about.com/od/typesofpsychotherapy/a/behavioral-therapy.htm
• http://www.psychologycampus.com/behavioral-psychology/
• http://psych.answers.com/behavioral/basic-principles-of-behaviorist-psychology
